|
Staff
Join Date: November 23, 2005
Location: California - San Francisco
Posts: 9,471
|
Quote:
|
Originally Posted by The_Doctor
...I saw a statistic a while back that no civilian had ever been killed in the US once they had put at least one .22 round into their assailant...
|
Really? Cite your source. I really don't believe it. Among other things, in 1986 Michael Lee Platt received a mortal wound from a 9mm and proceeded to kill or wound eight FBI agents.
So let's have a look at some real data and see why you're wrong.
There is data, and there are studies, and we have a good deal of knowledge about wound physiology, and none of it supports the notion that:
Quote:
|
Originally Posted by The_Doctor
...There are *very* few times when a .22 mag will be less effective, with identical shot placement, vs a 9mm or even a .357.....
|
What the data shows with regard to self defense could be summarized as follows:
- Pretty much every cartridge ever made has at times succeeded at quickly stopping an assailant.
- Pretty much every cartridge ever made has at times failed at quickly stopping an assailant.
- Considering ballistic gelatin performance, data available on real world incidents, an understanding of wound physiology and psychology, certain cartridges with certain bullets are more likely to be more effective more of the time.
- For defensive use in a handgun the 9mm Luger, .38 Special +P, .40 S&W, .45 ACP, .357 Magnum, and other, similar cartridges when of high quality manufacture, and loaded with expanding bullets appropriately designed for their respective velocities to both expand and penetrate adequately, are reasonably good choices.
- And that's probably as good as we can do.
I've posted the following before and might as well post it again here:
Let's consider how shooting someone will actually cause him to stop what he's doing.
- The goal is to stop the assailant.
- There are four ways in which shooting someone stops him:
- psychological -- "I'm shot, it hurts, I don't want to get shot any more."
- massive blood loss depriving the muscles and brain of oxygen and thus significantly impairing their ability to function
- breaking major skeletal support structures
- damaging the central nervous system.
Depending on someone just giving up because he's been shot is iffy. Probably most fights are stopped that way, but some aren't; and there are no guarantees.
Breaking major skeletal structures can quickly impair mobility. But if the assailant has a gun, he can still shoot. And it will take a reasonably powerful round to reliably penetrate and break a large bone, like the pelvis.
Hits to the central nervous system are sure and quick, but the CNS presents a small and uncertain target. And sometimes significant penetration will be needed to reach it.
The most common and sure physiological way in which shooting someone stops him is blood loss -- depriving the brain and muscles of oxygen and nutrients, thus impairing the ability of the brain and muscles to function. Blood loss is facilitated by (1) large holes causing tissue damage; (2) getting the holes in the right places to damage major blood vessels or blood bearing organs; and (3) adequate penetration to get those holes into the blood vessels and organs which are fairly deep in the body. The problem is that blood loss takes time. People have continued to fight effectively when gravely, even mortally, wounded. So things that can speed up blood loss, more holes, bigger holes, better placed holes, etc., help.
So as a rule of thumb --
- More holes are better than fewer holes.
- Larger holes are better than smaller holes.
- Holes in the right places are better than holes in the wrong places.
- Holes that are deep enough are better than holes that aren't.
- There are no magic bullets.
- There are no guarantees.
- With regard to the issue of psychological stops see
- this study, entitled "An Alternate Look at Handgun Stopping Power" by Greg Ellifritz. And take special notice of his data on failure to incapacitate rates:
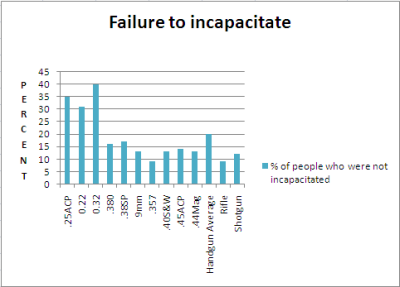
As Ellifritz notes in his discussion of his "failure to incapacitate" data (emphasis added):
Quote:
|
Originally Posted by Greg Ellifritz
...Take a look at two numbers: the percentage of people who did not stop (no matter how many rounds were fired into them) and the one-shot-stop percentage. The lower caliber rounds (.22, .25, .32) had a failure rate that was roughly double that of the higher caliber rounds. The one-shot-stop percentage (where I considered all hits, anywhere on the body) trended generally higher as the round gets more powerful. This tells us a couple of things...
In a certain (fairly high) percentage of shootings, people stop their aggressive actions after being hit with one round regardless of caliber or shot placement. These people are likely NOT physically incapacitated by the bullet. They just don't want to be shot anymore and give up! Call it a psychological stop if you will. Any bullet or caliber combination will likely yield similar results in those cases. And fortunately for us, there are a lot of these "psychological stops" occurring. The problem we have is when we don't get a psychological stop. If our attacker fights through the pain and continues to victimize us, we might want a round that causes the most damage possible. In essence, we are relying on a "physical stop" rather than a "psychological" one. In order to physically force someone to stop their violent actions we need to either hit him in the Central Nervous System (brain or upper spine) or cause enough bleeding that he becomes unconscious. The more powerful rounds look to be better at doing this....
|
- There are two sets of data in the Ellifritz study: incapacitation and failure to incapacitate. They present some contradictions.
- Considering the physiology of wounding, the data showing high incapacitation rates for light cartridges seems anomalous.
- Furthermore, those same light cartridges which show high rates of incapacitation also show high rates of failures to incapacitate. In addition, heavier cartridges which show incapacitation rates comparable to the lighter cartridges nonetheless show lower failure to incapacitate rates.
- And note that the failure to incapacitate rates of the 9mm Luger, .40 S&W, .45 ACP, and .44 Magnum were comparable to each other.
- If the point of the exercise is to help choose cartridges best suited to self defense application, it would be helpful to resolve those contradictions.
- A way to try to resolve those contradictions is to better understand the mechanism(s) by which someone who has been shot is caused to stop what he is doing.
- The two data sets and the apparent contradiction between them (and as Ellifritz wrote) thus strongly suggest that there are two mechanisms by which someone who has been shot will be caused to stop what he is doing.
- One mechanism is psychological. This was alluded to by both Ellifritz and FBI agent and firearms instructor Urey Patrick. Sometimes the mere fact of being shot will cause someone to stop. When this is the stopping mechanism, the cartridge used really doesn't matter. One stops because his mind tells him to because he's been shot, not because of the amount of damage the wound has done to his body.
- The other mechanism is physiological. If the body suffers sufficient damage, the person will be forced to stop what he is doing because he will be physiologically incapable of continuing. Heavier cartridges with large bullets making bigger holes are more likely to cause more damage to the body than lighter cartridges. Therefore, if the stopping mechanism is physiological, lighter cartridges are more likely to fail to incapacitate.
- And in looking at any population of persons who were shot and therefore stopped what they were doing, we could expect that some stopped for psychological reasons. We could also expect others would not be stopped psychologically and would not stop until they were forced to because their bodies became physiologically incapable of continuing.
- From that perspective, the failure to incapacitate data is probably more important. That essentially tells us that when Plan A (a psychological stop) fails, we must rely on Plan B (a physiological stop) to save our bacon; and a heavier cartridge would have a lower [Plan B] failure rate.
- Also see the FBI paper entitled "Handgun Wounding Factors and Effectiveness", by Urey W. Patrick. Agent Patrick, for example, notes on page 8:
Quote:
...Psychological factors are probably the most important relative to achieving rapid incapacitation from a gunshot wound to the torso. Awareness of the injury..., fear of injury, fear of death, blood or pain; intimidation by the weapon or the act of being shot; or the simple desire to quit can all lead to rapid incapacitation even from minor wounds. However, psychological factors are also the primary cause of incapacitation failures.
The individual may be unaware of the wound and thus have no stimuli to force a reaction. Strong will, survival instinct, or sheer emotion such as rage or hate can keep a grievously wounded individual fighting....
|
- And for some more insight into wound physiology and "stopping power":
- Dr. V. J. M. DiMaio (DiMaio, V. J. M., M. D., Gunshot Wounds, Elsevier Science Publishing Company, 1987, pg. 42, as quoted in In Defense of Self and Others..., Patrick, Urey W. and Hall, John C., Carolina Academic Press, 2010, pg. 83):
Quote:
|
In the case of low velocity missles, e. g., pistol bullets, the bullet produces a direct path of destruction with very little lateral extension within the surrounding tissue. Only a small temporary cavity is produced. To cause significant injuries to a structure, a pistol bullet must strike that structure directly. The amount of kinetic energy lost in the tissue by a pistol bullet is insufficient to cause the remote injuries produced by a high-velocity rifle bullet.
|
- And further in In Defense of Self and Others... (pp. 83-84, emphasis in original):
Quote:
|
The tissue disruption caused by a handgun bullet is limited to two mechanisms. The first or crush mechanism is the hole that the bullet makes passing through the tissue. The second or stretch mechanism is the temporary wound cavity formed by the tissue being driven outward in a radial direction away from the path of the bullet. Of the two, the crush mechanism is the only handgun wounding mechanism that damages tissue. To cause significant injuries to a structure within the body using a handgun, the bullet must penetrate the structure.
|
- And further in In Defense of Self and Others... (pp. 95-96, emphasis in original):
Quote:
|
Kinetic energy does not wound. Temporary cavity does not wound. The much-discussed "shock" of bullet impact is a fable....The critical element in wounding effectiveness is penetration. The bullet must pass through the large blood-bearing organs and be of sufficient diameter to promote rapid bleeding....Given durable and reliable penetration, the only way to increase bullet effectiveness is to increase the severity of the wound by increasing the size of the hole made by the bullet....
|
- And sometimes a .357 Magnum doesn't work all that well. LAPD Officer Stacy Lim who was shot in the chest with a .357 Magnum and still ran down her attacker, returned fire, killed him, survived, and ultimately was able to return to duty. She was off duty and heading home after a softball game and a brief stop at the station to check her work assignment. According to the article I linked to:
Quote:
|
... The bullet ravaged her upper body when it nicked the lower portion of her heart, damaged her liver, destroyed her spleen, and exited through the center of her back, still with enough energy to penetrate her vehicle door, where it was later found....
|
- But take special note of the quote in the third bullet point in item V., above:
- In In Defense of Self and Others... (pp. 95-96, with my emphasis):
Quote:
|
... the only way to increase bullet effectiveness is to increase the severity of the wound by increasing the size of the hole made by the bullet....
|
- So a sub-caliber, .22 lr, .25 ACP, or similar, can kill and can, under some circumstances, stop an attacker. But the odds are that something larger will be more likely to be effective. A sub-caliber might fill a special need, such as a need for deep concealment or if one can't handle something larger; but if someone has a choice, a sub-caliber will not be the best choice.
__________________
"It is long been a principle of ours that one is no more armed because he has possession of a firearm than he is a musician because he owns a piano. There is no point in having a gun if you are not capable of using it skillfully." -- Jeff Cooper
Last edited by Frank Ettin; January 4, 2015 at 07:16 PM.
|